CBS 2019





CBSMD教育中心




HOME


CBS 2019
At CBS






General Information
Association and Affiliations
Organized by
Nanjing Heart Center
Asian Bifurcation Club (ABC)
Nanjing First Hospital, Nanjing Medical University
Co-organized by
Chinese Society of Cardiology (CSC)
Capacity Building and Continuing Education Center,National Health and Family Planning Commission (CBCEC)
American Society for Cardiovascular Angiography and Interventions (SCAI)
Asian Heart Society (AHS)
Contact Us
Registration Administration of Domestic Representatives
Hongjuan Peng : +86-13913895477
+86-13913895477
Haimei Xu +86-13914736846
 cbsnj@cbsmd.cn
cbsnj@cbsmd.cn
Registration Administration of Overseas Representatives
Ling Lin : +86 (25) 52271398
+86-13951884596
cbs@cbsmd.cn
Management of Challenging Cases
Yingying Zhao :+86-13815408517
sub@cbsmd.cn
Address
 CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
 210006
210006


FACULTY
FACULTY
General Chairman
Congress Chairman


Education Center
Education Center
• Online Education (For more customized user interface with self-defined collection of research papers and education resources.)
• CBS Education Resource



• CBSMD Scientific Library




SCIENTIFIC LIBRARY
SCIENTIFIC LIBRARY
Research Paper
> Acute Coronary Syndrom
> ASCVD Prevention
> Bifurcation Stenting
> Cardio-Oncology
> Congestive Heart Failure
> DAPT Duration
> Drug Coated Balloon
> Fractional Flow Reserve
> IVUS Guidance
> Optical Coherence Tomography
> Pulmonary Hypertension
> Rotational Atherectomy
> Shear Stress
> Stenting Left Main
> Transcatheter Aortic Valve Replacement
> Percutaneous LAA Occlusion
> Mitral/Tricuspid Valvular Disease
> Other Relevant Articles
Recommended Paper
Management of Acute Myocardial Infarction During the COVID-19 Pandemic
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up
CSC Expert Consensus on Principles of Clinical Management of Patients with Severe Emergent Cardiovascular Diseases during the COVID-19 Epidemic
ACC Clinical Bulletin Focuses on Cardiac Implications of Coronavirus (COVID-19)
Pre-reading
Antithrombotic Strategy in Patients With AF and Recent ACS or PCI: Primary Results of the AUGUSTUS Trial
Amit N. Vora, MD, MPH; John H. Alexander, MD, FACC; Renato D. Lopes, MD, PHD, FACC
INTRODUCTION - The optimal antithrombotic strategy for patients with atrial
fibrillation (AF) with acute coronary syndrome (ACS) and/or recent
percutaneous coronary intervention (PCI) can be challenging. Although
dual antiplatelet therapy (DAPT) is indicated for secondary prevention
of coronary events and to protect against stent thrombosis, it is not
indicated for stroke prevention in patient with AF.1-3 Conversely, oral anticoagulation (OAC) with either warfarin or a direct
oral anticoagulant (DOAC) is indicated for stroke prevention in patients
with AF but provides limited protection against future coronary
ischemic events or stent thrombosis (although there are emerging data
demonstrating some benefit with DOACs).1,3,4 Furthermore, the
combination of antiplatelet and anticoagulant therapies (i.e., triple
therapy) has been associated with significantly increased risk of
bleeding and with less clear benefit with respect to ischemic events.5-7
PIONEER-AF PCI (An Open-Label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects With Atrial Fibrillation Who Undergo Percutaneous Coronary Intervention) randomized 2,100 patients to 3 strategies that included 2 rivaroxaban-based strategies and 1 traditional vitamin K antagonist (VKA) based triple therapy strategy and found lower rates of bleeding in the two rivaroxaban-based strategies compared with the VKA-based strategy.9 Likewise, the REDUAL PCI trial (Randomized Evaluation of Dual Antithrombotic Therapy With Dabigatran vs. Triple Therapy With Warfarin in Patients With Nonvalvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention) randomized 2,725 patients to 2 different doses of dabigatran with P2Y12 inhibitor versus a warfarin-based triple therapy strategy and found lower rates of bleeding with the dabigatran-based strategies.10
Whereas both of these studies demonstrated the safety of DOAC-based strategies, they were not designed to assess whether the observed bleeding reduction was due to the DOAC or simply the discontinuation of aspirin. Additionally, PIONEER-AF PCI studied doses of rivaroxaban that were not demonstrated to reduce stroke in patients with AF.
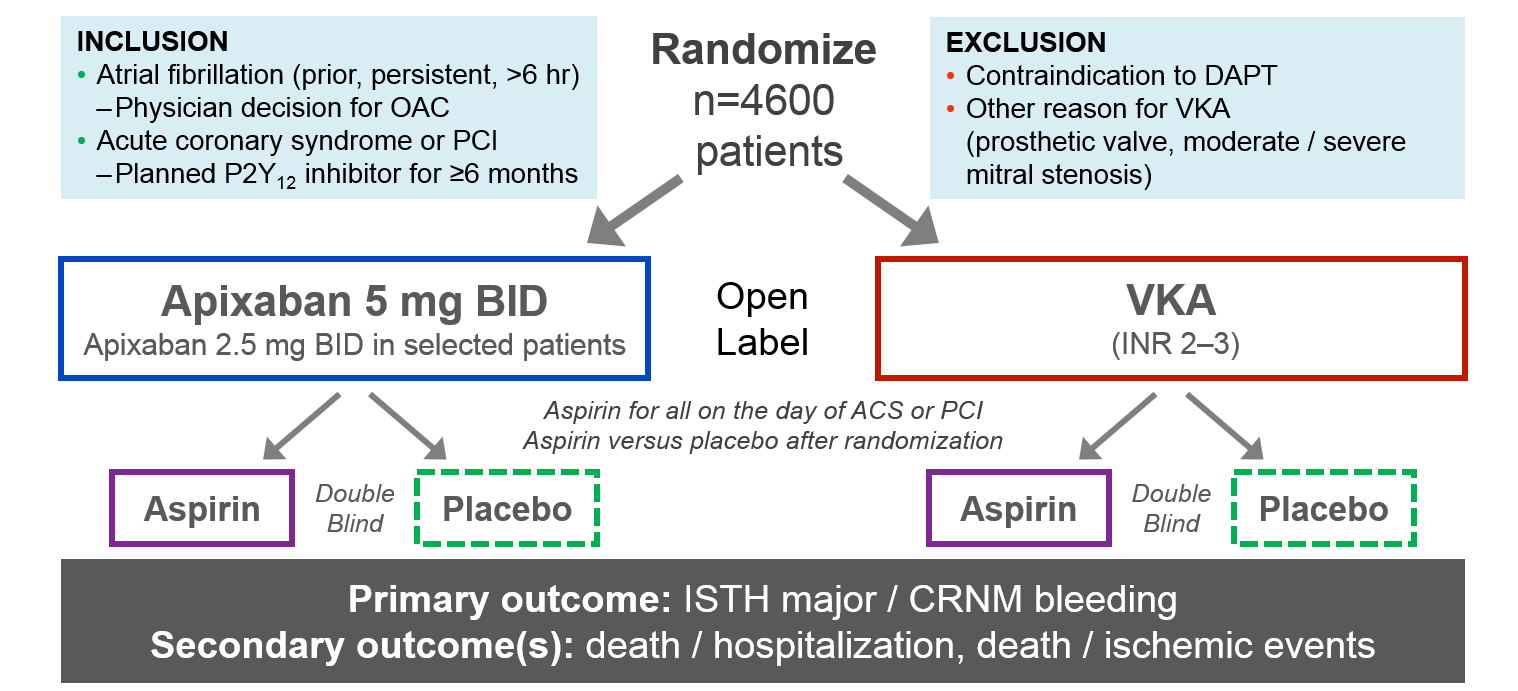
AUGUSTUS STUDY DESIGN - AUGUSTUS (Antithrombotic Therapy After Acute Coronary Syndrome or PCI in Atrial Fibrillation) is a 2 x 2 factorial randomized clinical trial that sought to determine the optimal antithrombotic strategy among patient with AF and recent ACS and/or PCI.11 Patients were assigned to either open-label warfarin or apixaban and double-blind aspirin or aspirin placebo on planned P2Y12 inhibitor. The trial was designed to test two independent hypotheses:
The primary outcome for each study factor was ISTH major/CRNM bleeding. The secondary outcome included death or hospitalization, death or ischemic events (stroke, myocardial infarction, stent thrombosis, urgent revascularization), and the individual components of the secondary outcomes. The study follow-up period was 6 months.
Figure 1 Study Flow of AUGUSTUS Trial
PRIMARY RESULTS OF AUGUSTUS - The study randomized 4,614 patients from 494 sites across 33 countries.12 The median age of all patients was 70.6 years, and about one-third of patients were women. Patient characteristics were well-balanced across study arms. The mean CHADS-VASc score was 3.9, and the mean HAS-BLED score was 2.9, indicating a high risk of ischemic stroke as well as bleeding. Only half of all patients had been on prior OAC, and 92.6% of patients were on clopidogrel, with the remainder on other P2Y12 agents.
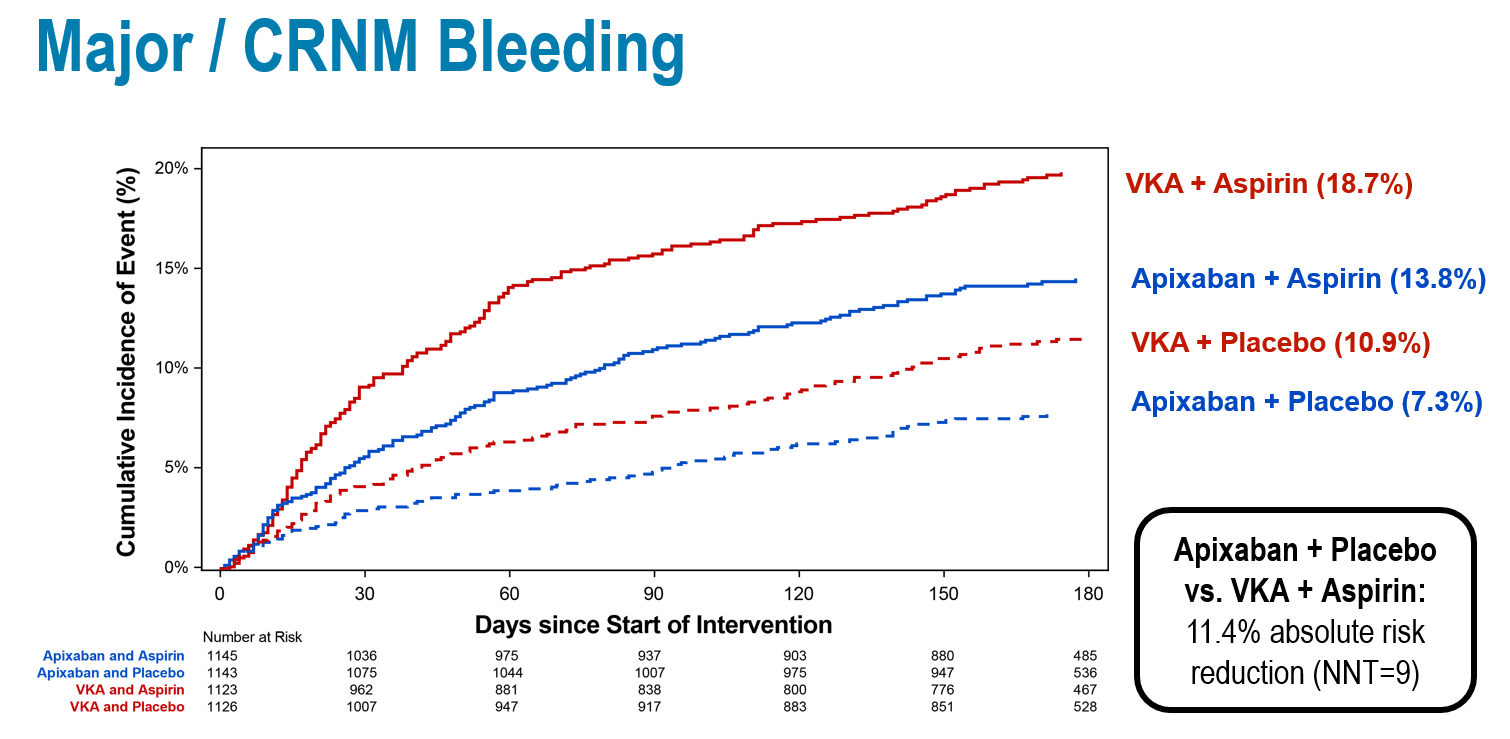
At 6 months, 10.5% of patients receiving apixaban and 14.7% receiving warfarin had an ISTH major/CRNM bleeding event (hazard ratio [HR] 0.69; 95% confidence interval [CI], 0.58-0.81), meeting the prespecified endpoints for both noninferiority and superiority. Among patients receiving aspirin, 16.1% had a bleeding event compared with 9.0% receiving aspirin placebo (HR 1.89; 95% CI, 1.59-2.24; p < 0.001). The number needed to treat (NNT) with apixaban compared with warfarin over 6 months to prevent 1 episode of bleeding was 24, whereas the number needed to harm with treatment using aspirin versus placebo was 14.
Apixaban was found to be superior to warfarin with respect to death/rehospitalization (23.5% vs. 27.4%) (HR 0.83; 95% CI, 0.74-0.96; p = 0.002; NNT = 26), driven primarily by differences in rates of rehospitalization. However, no such difference was observed in the antiplatelet-regimen comparison (26.2% with aspirin vs. 24.7% with aspirin placebo) (HR 1.08; 95% CI, 0.96-1.21).
With respect to death or ischemic events, there were no significant differences between apixaban/warfarin (6.7% vs 7.1%) (HR 0.93; 95% CI, 0.75-1.16) or aspirin/placebo (6.5% vs 7.3%) (HR 0.89; 95% CI, 0.71-1.11), though apixaban treatment resulted in fewer strokes (0.6% vs 1.1%) (HR 0.50; 95% CI, 0.26-0.97). Although the individual endpoints are exploratory and hypothesis generating, this provides additional reassurance about the importance of choosing the indicated dose of apixaban that has previously demonstrated stroke prevention.
Figure 2 Primary Outcome of AUGUSTUS Trial
CLINICAL IMPLICATIONS - AUGUSTUS is the first study to evaluate the independent effects of anticoagulant and antiplatelet therapy on patients with AF and recent ACS and/or PCI. The study found that apixaban resulted in lower bleeding compared with warfarin, and aspirin resulted in higher bleeding than placebo. Apixaban also resulted in lower rates of death/rehospitalization compared with warfarin, driven primarily by rehospitalization. For most patients, a regimen of aspirin on background clopidogrel offered balance between the ischemic and bleeding risks in this high-risk population.
Although not statistically significant, the study did demonstrate higher numerical counts of myocardial infarction, urgent revascularization, and stent thrombosis among patients assigned to placebo compared with patients assigned to aspirin. There are still questions to be answered about timing, predictors, and prognosis of stent thrombosis as well as the risk-benefit ratio between stent thrombosis and bleeding at different time points after the ACS/PCI event. This likely warrants further study.
However, AUGUSTUS clarifies the specific risks associated with the various treatment strategies and demonstrates that the risk of ischemic events is relatively low, even among patients assigned to aspirin. This suggests that a strategy of apixaban and clopidogrel without aspirin is safest for most patients, without significant differences in ischemic events compared with regimens that included a VKA, aspirin, or both.
Thus, one reasonable approach may be to use aspirin during the initial treatment of the ACS/PCI event and during the course of hospitalization. Aspirin can then be safely discontinued around the time of discharge and the OAC and P2Y12 inhibitor maintained for at least 6 months.
SUMMARY - In patients with AF and recent ACS and/or PCI who are treated on background P2Y12 inhibitor, an antithrombotic strategy of apixaban without concomitant aspirin use resulted in less bleeding and fewer hospitalizations with no statistically significant increase in ischemic events compared with a regimen of VKA and/or aspirin.
REFERENCES
2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Gui...
Heart Rhythm. | Jun 11,2019
An open-Label, 2 × 2 factorial, randomized controlled trial to evaluate the ...
Am J Cardiol. | Mar 12,2019
Rationale and design of the comParIson Of sacubitril/valsartaN versus Enal...
Am J Cardiol. | Mar 12,2019
Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibril...
N Engl J Med. | Sep 04,2017
Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing P...
N Engl J Med. | Jun 11,2019
2016 ACC/AHA guideline focused update on duration of dual antiplatelet the...
J Thorac Cardiovasc Surg. | Jun 11,2019
2014 AHA/ACC Guideline for the Management of Patients with Non-ST-...
J Am Coll Cardiol. | Nov 22,2018












 中 文
中 文











 CBS 2019
CBS 2019 CBS 2019 FACULTY
CBS 2019 FACULTY Education Resource
Education Resource CBSMD Scientific Library
CBSMD Scientific Library




