CBS 2019





CBSMD教育中心




HOME


CBS 2019
At CBS






General Information
Association and Affiliations
Organized by
Nanjing Heart Center
Asian Bifurcation Club (ABC)
Nanjing First Hospital, Nanjing Medical University
Co-organized by
Chinese Society of Cardiology (CSC)
Capacity Building and Continuing Education Center,National Health and Family Planning Commission (CBCEC)
American Society for Cardiovascular Angiography and Interventions (SCAI)
Asian Heart Society (AHS)
Contact Us
Registration Administration of Domestic Representatives
Hongjuan Peng : +86-13913895477
+86-13913895477
Haimei Xu +86-13914736846
 cbsnj@cbsmd.cn
cbsnj@cbsmd.cn
Registration Administration of Overseas Representatives
Ling Lin : +86 (25) 52271398
+86-13951884596
cbs@cbsmd.cn
Management of Challenging Cases
Yingying Zhao :+86-13815408517
sub@cbsmd.cn
Address
 CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
 210006
210006


FACULTY
FACULTY
General Chairman
Congress Chairman


Education Center
Education Center
• Online Education (For more customized user interface with self-defined collection of research papers and education resources.)
• CBS Education Resource



• CBSMD Scientific Library




SCIENTIFIC LIBRARY
SCIENTIFIC LIBRARY
Research Paper
> Acute Coronary Syndrom
> ASCVD Prevention
> Bifurcation Stenting
> Cardio-Oncology
> Congestive Heart Failure
> DAPT Duration
> Drug Coated Balloon
> Fractional Flow Reserve
> IVUS Guidance
> Optical Coherence Tomography
> Pulmonary Hypertension
> Rotational Atherectomy
> Shear Stress
> Stenting Left Main
> Transcatheter Aortic Valve Replacement
> Percutaneous LAA Occlusion
> Mitral/Tricuspid Valvular Disease
> Other Relevant Articles
Recommended Paper
Management of Acute Myocardial Infarction During the COVID-19 Pandemic
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up
CSC Expert Consensus on Principles of Clinical Management of Patients with Severe Emergent Cardiovascular Diseases during the COVID-19 Epidemic
ACC Clinical Bulletin Focuses on Cardiac Implications of Coronavirus (COVID-19)
Pre-reading
The 6th World Symposium on PH: Hemodynamic Definitions and Updated Clinical Classification of PH
Saurabh Rajpal, Steven Stroud, Sophia Elizabeth Airhart, Veronica Franco, Riaz Rahman, Manreet Kanwar, Sasha Prisco, Kurt Prins
The 6th World Symposium on Pulmonary Hypertension proposed some fundamental changes to the hemodynamic and clinical classification of pulmonary hypertension (PH). We have summarized these changes below.
Change in Criteria for Diagnosis of PH - Based on the mean pulmonary artery pressure (mPAP) of 20 mmHg being 2 standard deviations above the mean value of 14.0 ± 3.3 mmHg, which was the normal value of mPAP observed in recent published data, and the fact that there have been multiple studies across different clinical types of PH documenting poor outcomes in patients with mPAP between 20 and 25 mmHg, it was proposed to define PH as mPAP >20 mmHg instead of mPAP ≥25 mmHg at rest, measured by right heart catheterization.
Pulmonary Vascular Resistance (PVR) Added to Definition of all Forms of Pre-Capillary PH - To identify pre-capillary PH as representative of pulmonary vascular disease, it was proposed to include PVR of ≥3 Wood units in the definition of all forms of pre-capillary PH associated with mPAP >20 mmHg.
Combined Pre- and Post-Capillary PH - The cutoff of ≥3 Wood units was also proposed to identify the group of patients that has combined pre- and post-capillary PH in addition to the mandatory pulmonary capillary wedge pressure of >15 mmHg and mPAP >20 mmHg, which is a prerequisite to be classified as having any type of post-capillary PH. This group of patients has worse prognosis compared with other patients with post-capillary PH.
Exercise PH - A definition for exercise PH could not reintroduced. The challenges of getting accurate right heart catheterization measurements and the lack of diagnostic discrimination power whether exercise PH is due to elevated pulmonary capillary wedge pressure (left heart disease) or pulmonary vascular disease makes it difficult to define exercise PH as an entity.
Drug- or Toxin-Associated PH - Drugs and toxins were divided into those with definitive association (epidemiologic outbreaks, case control and randomized control trials; e.g., dasatinib and methamphetamines) and those with possible association (e.g., cocaine).
Pulmonary Arterial Hypertension Long-Term Responders to Calcium Channel Blockers - These patients were introduced as a distinct group within Group I because they have been shown to have significantly better prognosis, unique management, and different pathophysiology. These patients are defined by a reactive vasodilators stress (a reduction of mPAP ≥10 mmHg to reach an absolute value of mPAP ≤40 mmHg with an increased or unchanged cardiac output) and a sustained hemodynamic response a year after being on calcium channel blockers and New York Heart Association Functional Class I/II.
Pulmonary Veno-occlusive Disease/Pulmonary Capillary Hemangiomatosis - These were defined as pulmonary arterial hypertension with overt features of venous/capillaries involvement was included in World Health Organization (WHO) Group I because their clinical presentation and hemodynamic profile are similar to PH.
WHO Group 4 Updates: PH due to Pulmonary Artery Obstructions - In addition to chronic thromboembolic PH, the entities included in this group were expanded to include other etiologies of pulmonary artery obstruction such as congenital pulmonary artery stenosis (Alagille syndrome) and malignant and non-malignant tumors.
WHO Group 5 Simplified - In the WHO Group 5 group, splenectomy and thyroid disease was removed as a subgroup and is considered as more of a risk factor for PH. Lymphangioleiomyomatosis was reclassified as WHO Group 3 because almost all cases of PH in lymphangioleiomyomatosis are associated with only mild PH but severe pulmonary parenchymal disease.
Table 1: Updated Hemodynamic Definition of PH

Pulmonary hypertension (PH) due to left heart disease is a complex condition encompassing different clinical phenotypes, pathophysiology, and prognoses. In an effort to clarify the disease process and provide clinical guidance, Vachiéry et al. propose a simplified phenotypic and hemodynamic approach in light of recent literature findings.
PH due to left heart disease is defined as elevated pulmonary pressure in response to elevated left atrial pressure. Elevated left-sided pressures can result from different pathologies, but generally speaking, left heart disease comprises three groups:
Among these subsets, PH can exist as the following:
Consistent acquisition of key components during invasive hemodynamic testing with right heart catheterization remains challenging. Also, there is considerable difficulty delineating PH due to left heart disease from pulmonary arterial hypertension (PAH) with HFpEF because PAH patients often have concurrent cardiovascular disease. As such, the authors propose a three-phenotype classification system to refine PH due to left heart disease pre-test probability and stratify which patients require additional invasive studies (Figure 1):
Figure 1: Pre-Test Probability of PH due to Left Heart Disease Based on Clinical Phenotype
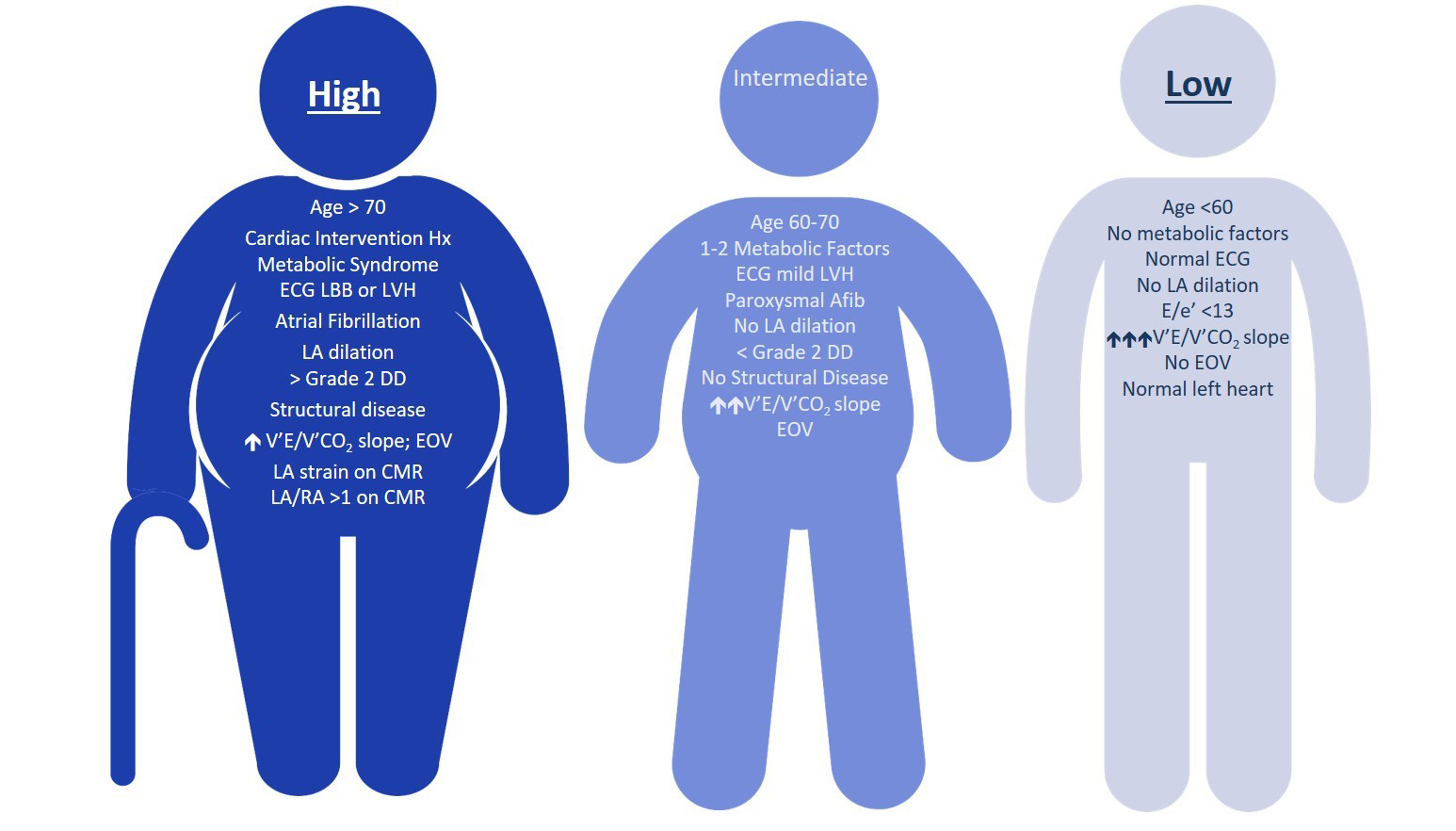
Resting Hemodynamic Evaluation of PH due to Left Heart Disease - If a patient exhibits an appropriate phenotype to warrant invasive hemodynamic studies, the following are proposed:
Provocative Hemodynamics - In patients with resting PAWP 13-15 mmHg and high/intermediate probability of PH with HFpEF, provocative testing should be considered to uncover PH due to HFpEF:
Calculations
Prognostic Factors
Treatment of PH due to Left Heart Disease
PH in Patients With End-Stage Heart Failure
Chronic thromboembolic pulmonary hypertension (CTEPH) (World Health Organization Group 4) is defined as follows:
The precise pathogenesis of CTEPH remains unclear but appears to be incited by acute pulmonary embolism with resultant altered vascular remodeling and endothelial dysfunction in the pulmonary arterial system. Chronic thromboembolic disease is characterized by similar symptoms and perfusion defects but without pulmonary hypertension at rest. CTEPH is an underdiagnosed condition that often presents with non-specific symptoms and requires a high index of clinical suspicion. Lung ventilation/perfusion scintigraphy is the screening test of choice; however, this test is infrequently ordered despite guideline recommendations.
Diagnosis is made by the following:
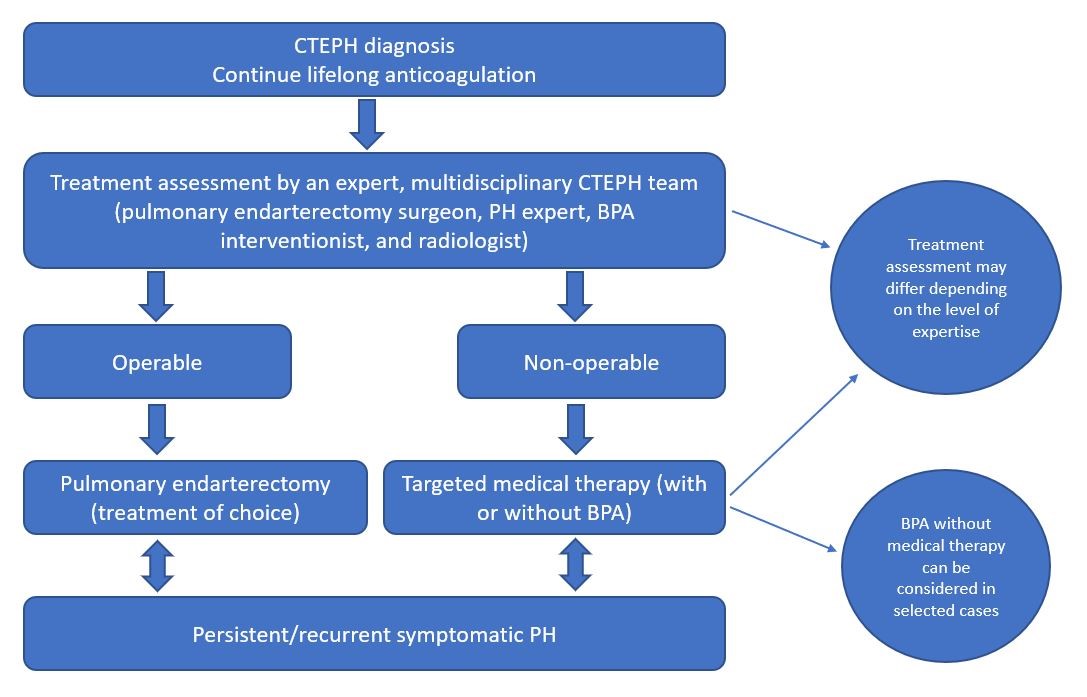
Treatment
Summary - Pulmonary endarterectomy remains the treatment of choice for operable CTEPH. For those deemed inoperable, the best level of evidence supports initiation of medical therapy and consideration for BPA.
Figure 1: CTEPH Revised Treatment Algorithm
Chronic lung disease-associated pulmonary hypertension (PH) is associated with reduced functional ability, impaired quality of life, greater oxygen requirements, and increased risk of mortality compared with patients with chronic lung disease. At this time, it is uncertain whether the presence of PH is causative or a surrogate of worse outcomes in chronic lung disease. However, patients with chronic lung disease-associated PH have the worst outcomes of all patients with PH.
Screening for PH in Chronic Lung Disease - Elevated plasma levels of brain natriuretic peptide and N-terminal pro-brain natriuretic peptide may increase suspicion for PH. Echocardiography is the best noninvasive modality to screen for chronic lung disease-associated PH. Ratio of main pulmonary artery to ascending aorta >1 may also predict PH.
Diagnosis - Right heart catherization is the gold standard for diagnosis of chronic lung disease-associated PH, but suspicion for underlying PH does not mandate the completion of right heart catherization, especially if the right heart catherization results will not influence therapy or management decisions, including referral for transplantation. Right heart catherization may be considered when clinical worsening, progressive exercise limitation and/or gas exchange abnormalities are not deemed attributable to ventilatory impairment and an accurate prognostic assessment is considered important. There are no valid data to support the routine use of acute vasodilator testing in chronic lung disease-associated PH.
Hemodynamic Definition - Chronic lung disease with PH is defined as mean pulmonary arterial pressure (mPAP) = 21-24 mmHg with pulmonary vascular resistance ≥3 Wood units or mPAP = 25-34 mmHg. Chronic lung disease with severe PH is defined as mPAP ≥35 mmHg or mPAP ≥25 mmHg with low cardiac index (<2.0 L•min−1•m−2).
Treatment - Currently, there are no strong data proving pulmonary arterial hypertension-specific therapy improves outcomes in chronic lung disease-associated PH. It is recommended that these patients be referred to expert centers for further treatment options.












 中 文
中 文











 CBS 2019
CBS 2019 CBS 2019 FACULTY
CBS 2019 FACULTY Education Resource
Education Resource CBSMD Scientific Library
CBSMD Scientific Library




