CBS 2019





CBSMD教育中心




HOME


CBS 2019
At CBS






General Information
Association and Affiliations
Organized by
Nanjing Heart Center
Asian Bifurcation Club (ABC)
Nanjing First Hospital, Nanjing Medical University
Co-organized by
Chinese Society of Cardiology (CSC)
Capacity Building and Continuing Education Center,National Health and Family Planning Commission (CBCEC)
American Society for Cardiovascular Angiography and Interventions (SCAI)
Asian Heart Society (AHS)
Contact Us
Registration Administration of Domestic Representatives
Hongjuan Peng : +86-13913895477
+86-13913895477
Haimei Xu +86-13914736846
 cbsnj@cbsmd.cn
cbsnj@cbsmd.cn
Registration Administration of Overseas Representatives
Ling Lin : +86 (25) 52271398
+86-13951884596
cbs@cbsmd.cn
Management of Challenging Cases
Yingying Zhao :+86-13815408517
sub@cbsmd.cn
Address
 CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
CBS2019 Congress Secretariat, Nanjing First Hospital, Building No.9 68# Changle Road, Nanjing, China
 210006
210006


FACULTY
FACULTY
General Chairman
Congress Chairman


Education Center
Education Center
• Online Education (For more customized user interface with self-defined collection of research papers and education resources.)
• CBS Education Resource



• CBSMD Scientific Library




SCIENTIFIC LIBRARY
SCIENTIFIC LIBRARY
Research Paper
> Acute Coronary Syndrom
> ASCVD Prevention
> Bifurcation Stenting
> Cardio-Oncology
> Congestive Heart Failure
> DAPT Duration
> Drug Coated Balloon
> Fractional Flow Reserve
> IVUS Guidance
> Optical Coherence Tomography
> Pulmonary Hypertension
> Rotational Atherectomy
> Shear Stress
> Stenting Left Main
> Transcatheter Aortic Valve Replacement
> Percutaneous LAA Occlusion
> Mitral/Tricuspid Valvular Disease
> Other Relevant Articles
Recommended Paper
Management of Acute Myocardial Infarction During the COVID-19 Pandemic
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up
CSC Expert Consensus on Principles of Clinical Management of Patients with Severe Emergent Cardiovascular Diseases during the COVID-19 Epidemic
ACC Clinical Bulletin Focuses on Cardiac Implications of Coronavirus (COVID-19)
Pre-reading
Minimalist Approaches to TAVR: Options and Implications
Sandra Lauck, PhD, RN; Janarthanan Sathananthan; David Alexander Wood, MD, FACC; John G. Webb, MD, FACC
The way we care for patients undergoing transcatheter aortic valve replacement (TAVR) is rapidly evolving. Over the span of the last 5 years, early historical clinical practices informed by cardiac surgery have come under increased clinical and scientific scrutiny.1-3 As new evidence continues to emerge, there is a worldwide shift to a more minimalist approach that is better matched to contemporary technology, procedural approaches, patients' needs, and sustainable health services delivery.
What Does Minimalist Mean?
There is no consensus definition of how the multiple components of
care—from patients' admission to their discharge home—can be minimized
to achieve optimal outcomes. Rather, there is significant nuance in how
many programs are recalibrating their TAVR clinical pathways in the
spirit of adopting a less-invasive approach: "doing less to achieve more
and better." The term minimalist TAVR is often used in its
most limited interpretation to describe the avoidance of general
anesthesia in favor of alternative strategies that range widely from
deep sedation under surgical-like conditions to local anesthesia that is
more akin to cardiac catheterization practice.4-6 This
variability in definitions for what constitutes minimalist TAVR has
produced heterogeneous single-center studies and created challenges in
assessing the literature.
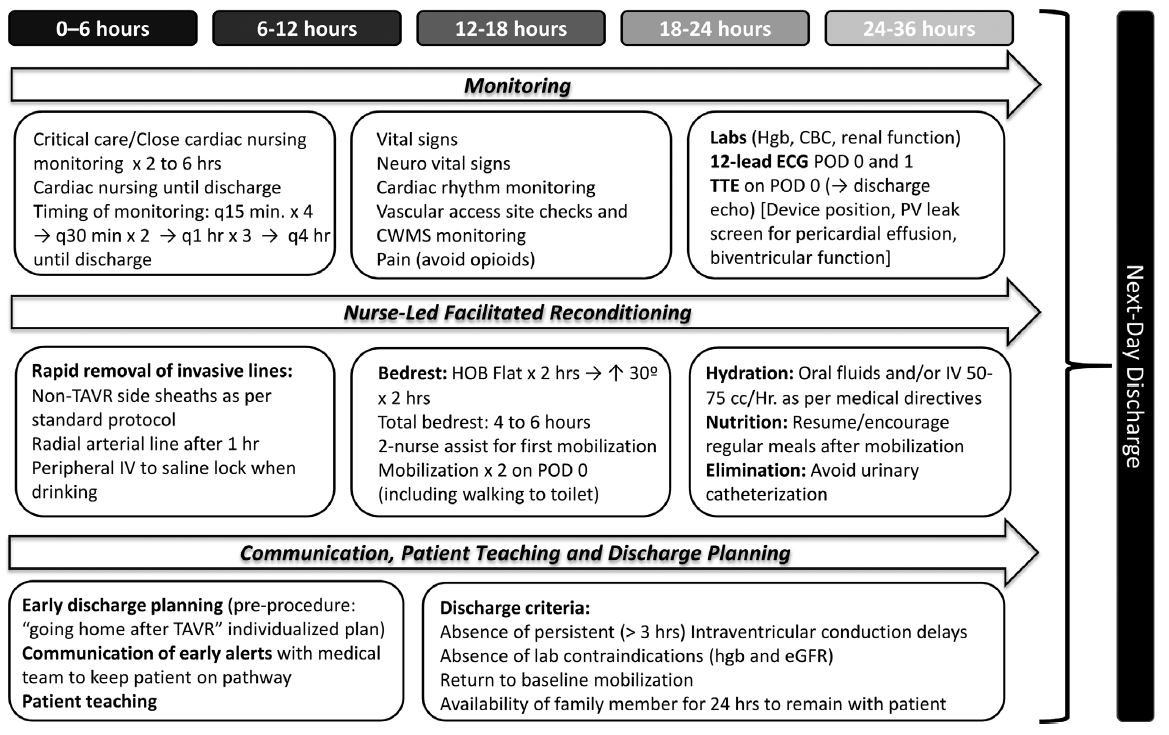
The Vancouver TAVR Clinical Pathway adopted a comprehensive approach of close scrutiny of all aspects of care (Figure 1).7 The safety and reproducibility of this clinical pathway was tested in the 3M TAVR (The Multidisciplinary, Multimodality, But Minimalist Approach to Transfemoral Transcatheter Aortic Valve Replacement) study in collaboration with 13 North American low-, medium-, and high-volume centers.8 The 3M TAVR study was the first and, to our knowledge, only study to date that prospectively assessed a consistent approach to minimalist TAVR to determine if a pathway inclusive of all components of patient care could be implemented across multiple and diverse centers. In this study, minimalist was operationalized as a series of best practices, including same-day admission for a procedure performed in a hybrid operating room or cardiac catheterization laboratory, avoidance of invasive lines (e.g., central venous and urinary catheters), local anesthesia only or with light procedural sedation administered by an anesthesiologist, percutaneous access and closure, and removal of the temporary pacemaker at the end of the procedure. The minimalist concept was further extended to the post-procedure phase, with a focus on rapid reconditioning, active mobilization after 4 hours, and accelerated return to baseline function and activities of daily living driven by a nursing protocol (Figure 2).9 The implementation of this standardized and highly optimized clinical pathway resulted in safe next-day discharge home of 80.1% of participants, and 89.5% were discharged within 48 hours. Importantly, outstanding results were achieved in the safety endpoints, with 2.9% composite mortality or stroke and 5.7% 30-day cardiac readmission.8
Figure 1
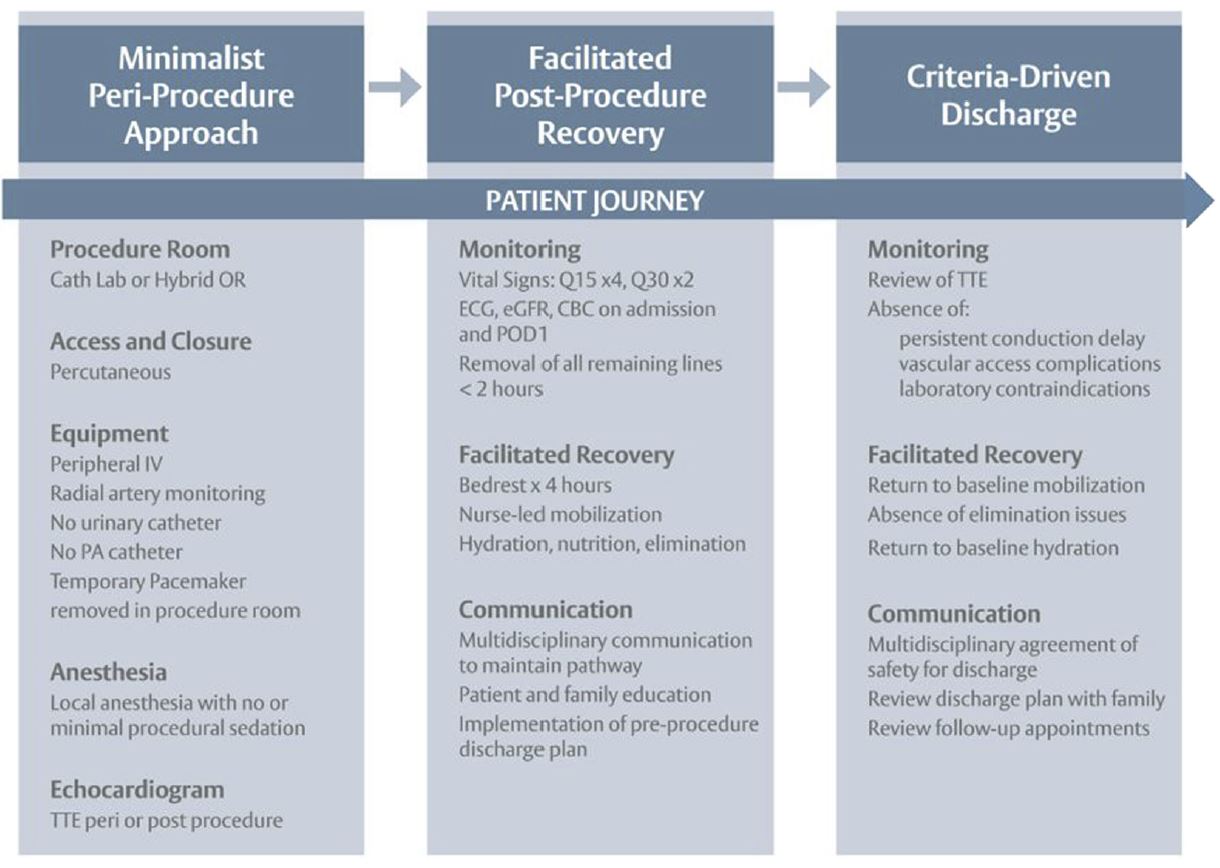
The 3M TAVR study demonstrated that a truly minimalist TAVR strategy that aims to achieve excellent outcomes was facilitated by 1) a multidisciplinary approach inclusive of all clinicians involved throughout patients' journeys of care; 2) a readiness for change; and 3) the adoption of a series of best practices that guided pre-, peri-, and post-procedure care for all patients. The Benchmark Program (Edwards Lifesciences; Irvine, CA) builds on the findings of the 3M TAVR study. This knowledge-translation initiative expands this evidence-based pathway on a global scale. The goals of the Benchmark Program are to deliver a standardized, reproducible, and scalable care pathway that helps TAVR programs achieve consistently excellent outcomes and patient experiences and improve access to care without increasing costs. The Benchmark Best Practices span the pre-, peri-, and post-procedure journey of care and require strong multidisciplinary engagement, continuous quality improvement, momentum for change, and commitment to seamless continuity of care.
Minimalist TAVR: Clinical Implications
The safe implementation of a minimalist TAVR protocol necessitates a
programmatic emphasis on "doing it right every time," with the goal of
attending to all details of patients' short journeys of in-hospital
care, avoiding even minor complications or set-backs, and achieving
consistently excellent outcomes without compromising patient safety.
There is evidence that predictable hemostasis and significant reduction in vascular injury can be achieved with ultrasound-guided vascular access, percutaneous closure, and activated clotting time monitoring.10 Accelerated mobilization and reconditioning are pivotal to avoiding a cascade of in-hospital adverse events in older patients, including loss of motor function and increased risk of falls.11 Similarly, the avoidance of hospitalization-related modifiable risk factors such as the use of general anesthesia and "deep" monitored anesthesia care, administration of opioids, urinary tract and other infections, immobility, deconditioning, and long length of stay (LOS) may reduce the incidence of procedure-related delirium to its near elimination in the era of contemporary TAVR.12,13 This contrasts sharply with the findings of a recent meta-analysis in which post-operative delirium after TAVR was identified in 8.1% of patients and was associated with significantly increased long-term mortality (odds ratio 2.1; confidence interval 1.2–3.7; p = 0.009).14 A final example of the core components of minimalist TAVR is the emphasis placed on early and ongoing discharge planning and attending to the potentially vulnerable phase of safe transition home. Consistent communication on the part of all health care providers about the target of next-day discharge home helps drive processes of care for clinicians (e.g., completion of post-procedure echocardiography, return to baseline mobilization, patient teaching) and enables patients and families to prepare their tailored discharge plan.9,15 Importantly, LOS and rates of early discharge must be considered in combination with incidence of 30-day readmission because procedural success is not only when the patient goes home, but also when the patient is able to stay home.
Although there is significant evidence that a minimalist approach is a safe default strategy for most patients, it may not be appropriate in all circumstances. The occurrence of a new conduction disturbance may signal the need for a longer admission to critical care, additional in-hospital investigations and interventions, and longer hospital LOS.16 The consideration of baseline electrocardiogram and varying rates of new permanent pacemaker across TAVR platforms may be important considerations that affect clinical requirements and early discharge. There is emerging evidence that select patients may benefit from undergoing an electrophysiology study and/or Holter or other heart rhythm device monitoring.17 Similarly, the role of transesophageal echocardiography to mitigate the risk of paravalvular leak remains debated. In recently published clinical trials of low surgical risk patients, the preferred use of conscious sedation for TAVR (PARTNER 3 [Placement of Aortic Transcatheter Valves 3]: 65.1%) was not associated with higher rates of moderate or severe paravalvular regurgitation.18 Future research will continue to inform how a minimalist strategy can be tailored to the unique needs of TAVR patients and technology.
Minimalist TAVR: Economic Opportunities
The chief drivers of TAVR costs include device price, management of in-hospital complications, and duration of hospitalization.19 Median LOS in the United States remains 3-5 days.20 LOS is a surrogate indicator of the cumulative effect of multiple
factors, including patient characteristics and risk profiles,
peri-procedure complications (e.g., new conduction delay), and
post-procedure care, as well as local protocols, processes of care, and
hospital culture. The reduction of post-procedure LOS offers
considerable opportunities for TAVR programs to curb costs, increase
capacity, and improve access to care and outcomes. In a recent
retrospective observation cohort study of nearly 15,000 fee-for-service
Medicare beneficiaries who underwent elective, uncomplicated
transfemoral TAVR in 2016, there was significant heterogeneity in LOS
across US centers, ranging from 1-2 days (49.8%) to 4 days and longer
(26.8%), that was primarily nested as in-hospital effects reflecting
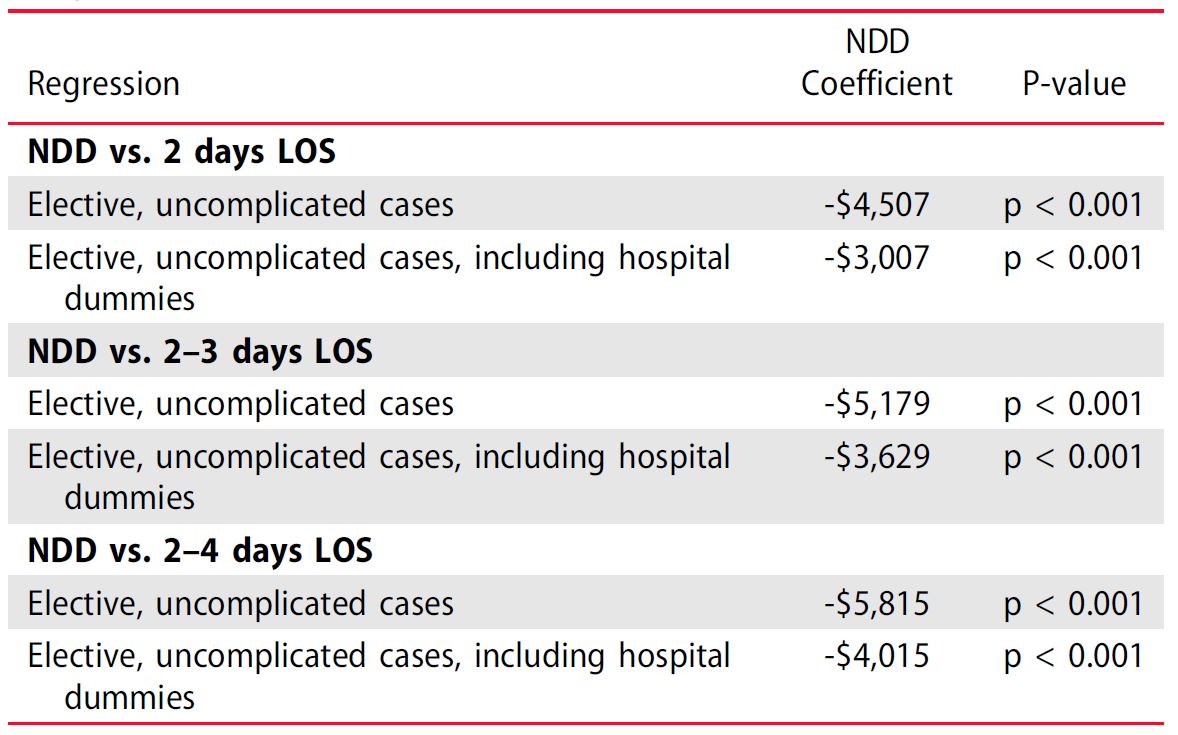
local practices. The adjusted cost for next-day discharge (NDD) was
nearly $7,500 lower compared with non-NDD (p < 0.001) and $5,200 when controlling for hospital fixed effects (p < 0.001) (Table 1). Estimated 2016 total cost savings ranged from $6,500,000 to $16,300,000 across the US system of care delivery.21
It is exceedingly difficult to quantify the totality of variables associated with LOS. In the emerging era of minimalist TAVR, there is a pressing need to investigate cost savings associated with the transition from historical practices to contemporary streamlined care. For example, the potentially more nimble and flexible use of a cardiac catheterization laboratory staffed with a core group of nurses and allied health professionals with expertise in structural heart intervention may afford significant savings compared with the mobilization of a full surgical team and its associated equipment and processes. Similarly, the transition to a preferred strategy of local anesthesia and light sedation, avoidance of invasive lines, reduced use of critical care facilities, and adoption of other minimalist TAVR best practices are likely to yield savings across programs of varying size and experience that are not fully captured in the study of cost of LOS.
Conclusion
The opportunities presented by enhanced technology, emerging evidence,
and programs' commitment to quality improvement have created a new
benchmark for the quality and cost of care of TAVR patients. The
transition to minimalist TAVR must be interpreted as the comprehensive
implementation of best practices that match patients' journeys of care
and involve the expertise of clinicians and administrators who
collectively contribute to all aspects of the TAVR clinical pathway. To
this end, we propose the following definition.
Minimalist TAVR refers to a fully optimized multidisciplinary clinical pathway that is grounded in evidence, adapted to the local context of care, and monitored through ongoing quality assurance. The pathway includes the following components:
Efforts to create a new standard of care are particularly salient in the era of expanded indications and the availability of TAVR to low-risk patients18,22 for whom expectations of consistently excellent results, rapid recovery, return to professional and other activities, avoidance of complications, and affordability of health services will continue to demand the highest standard of optimized and safe care.
References












 中 文
中 文











 CBS 2019
CBS 2019 CBS 2019 FACULTY
CBS 2019 FACULTY Education Resource
Education Resource CBSMD Scientific Library
CBSMD Scientific Library




